Answer of May 2025
For completion of the online quiz, please visit the eHKAM LMS website.
Clinical History:
A 96-year-old lady with unremarkable past health undergone a elective CT for non-specific abdominal pain, with incidental finding of a right groin mass.
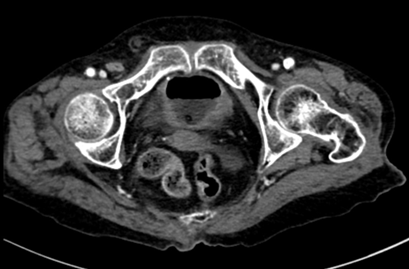
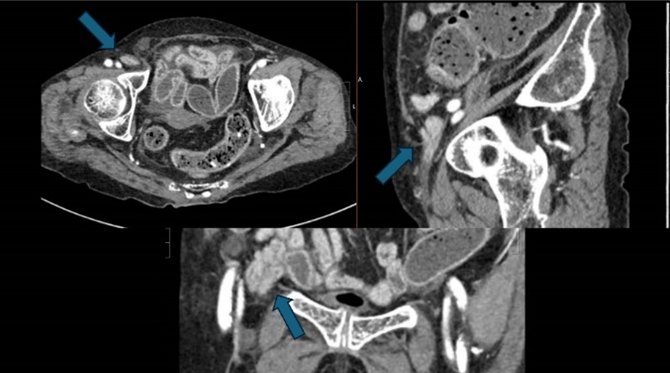
CT axial with contrast
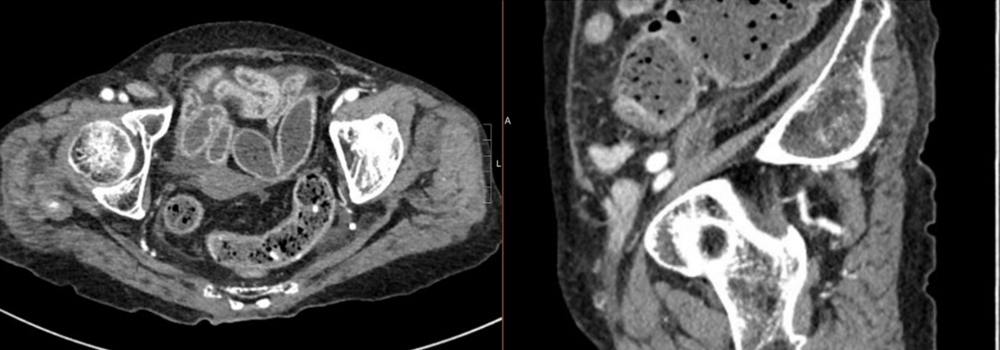
Multiplanar CT with contrast
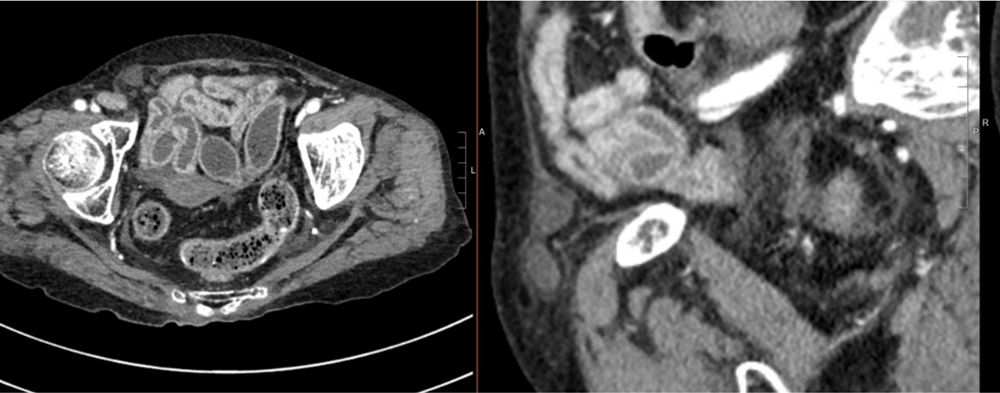
Multiplanar CT with contrast
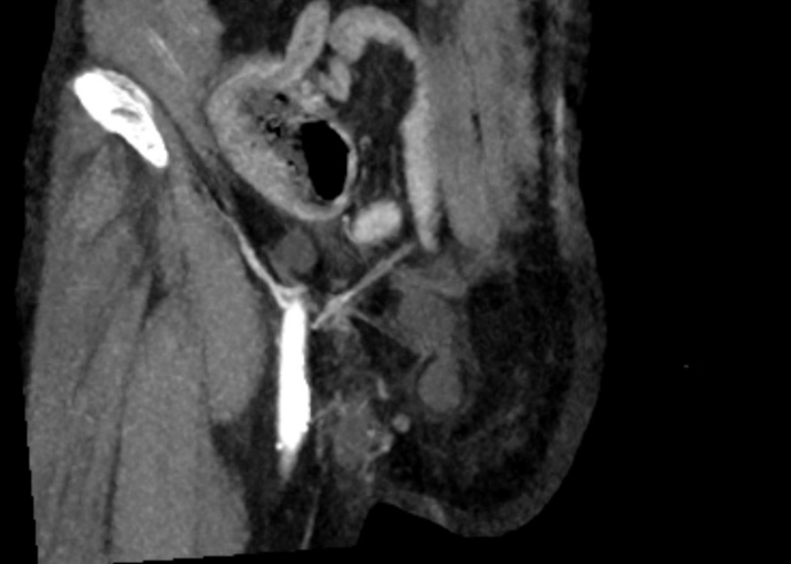
Coronal oblique MIP
DIAGNOSIS
Right Pantaloon hernia (concomitant right direct and indirect inguinal hernia)
IMAGING FINDINGS AND DISCUSSION


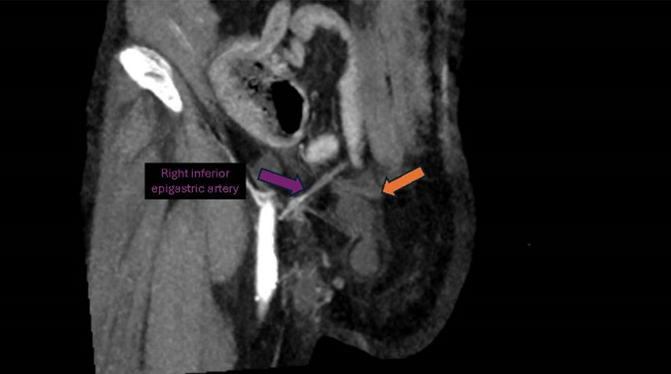
CT imaging demonstrates a right pantaloon hernia, characterized by the presence of two distinct hernia sacs in the right inguinal region, with their neck separated by inferior epigastric artery (indicated by the purple arrow):
1. Medial Hernia Sac (indicated by the orange arrow):
A fluid-filled hernia sac with its neck located medial to the inferior epigastric artery, consistent with a right direct inguinal hernia.
2. Lateral Hernia Sac (indicated by the blue arrow):
A hernia sac containing a segment of small bowel is identified, with its neck positioned lateral to the inferior epigastric artery, consistent with a right indirect inguinal hernia.
The coexistence of direct and indirect hernias within the same inguinal region is characteristic of a pantaloon hernia.
No evidence of bowel obstruction, strangulation, or ischemia is observed in this asymptomatic patient. No evidence of femoral vein compression to suggest the presence of femoral hernia.
Hernias of the groin have been reported to affect more than 18 million people worldwide. In this case, a 96-year-old female was incidentally found to have a pantaloon hernia on CT imaging. Pantaloon hernia, also known as saddle-bag or dual hernia, is a rare type of inguinal hernia characterized by the coexistence of both direct and indirect hernia sacs on either side of the inferior epigastric artery (IEA).
A thorough understanding of the detailed anatomic relationships in the inguinal region on CT images is critical to the diagnosis and differentiation of the three main types of hernias in this region. The course of the inferior epigastric vessels as well as the common femoral vein are critical landmarks, as their relationship to the hernia neck will determine the type of hernia.
The Hesselbach triangle is anatomically defined medially by the rectus abdominis muscle, superolaterally by the inferior epigastric vessels, and inferiorly by the inguinal ligament. The inferior epigastric artery arises from the external iliac artery immediately above the inguinal ligament, passes obliquely upward along the medial margin of the internal inguinal ring, and eventually anastomoses above the umbilicus with the superior epigastric artery . Knowledge of this anatomy is essential for recognizing hernia types and their relationship to these critical landmarks.
For radiologists, understanding the anatomy of the IEA and its relationship to hernia classification is critical. The course of the IEA is critical for distinguishing between direct and indirect hernias, with direct hernias occurring medial and indirect hernias lateral to this vascular landmark. Correct and prompt identification of Pantaloon hernia on imaging is crucial, as failure to recognize the indirect sac, which is often smaller and more subtle, can lead to misdiagnosis or incomplete surgical repair, increasing the risk of recurrence. Multiplanar reformatted (MPR) images allows for precise localization of the hernia sac in relation to the IEA and plays a fundamental role in the diagnosis of the type of hernia.
In this case, the incidentally detected pantaloon hernia demonstrates the importance of assessing the groin hernia with a systematic approach on CT, particularly in elderly patients or those undergoing imaging for other indications.