Answer of March 2024
For completion of the online quiz, please visit the eHKAM LMS website.
Clinical History:
A 61-year-old gentleman complains of upper limb involuntary movement for 2 weeks. He is a smoker, with a history of hyperlipidemia and Type 2 diabetes mellitus.
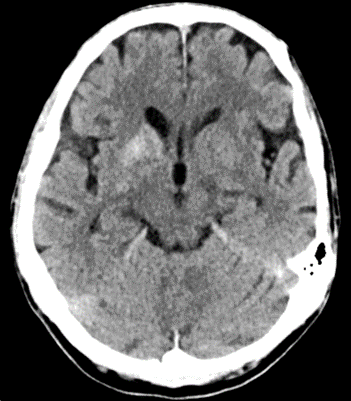
CT brain plain – axial

MRI brain T1W plain – axial
DIAGNOSIS:
Non-ketotic hyperglycemia hemichorea
DISCUSSION:
Non-ketotoic hyperglycemia hemichorea, also known as diabetic straitopathy, is a neurological complication of non-ketotic hyperglycemia. It is believed to be most common amongst Asian elderly women with poorly controlled diabetes. As the name suggests, the patient would classically be presented with unilateral involuntary choreiform movements, contralateral to the side of basal ganglia abnormalities seen under imaging.
MRI would be the modality of choice for diagnosis since CT brain could be initially normal. Signal abnormality would be seen in the striatal region (i.e. the caudate and putamen). T1W hyperintensity of caudate and putamen would be the most typical MRI finding. Increased susceptibility may also be seen under diffusion weighted imaging. T2W / FLAIR signal could be variable.
High density in the contralateral striatum of the affected limb would be seen under CT, typically later in the disease process.
Treatment of non-ketotoic hyperglycemia hemichorea would usually include management of patient’s hyperglycemia and use of dopamine receptor antagonists. Prognosis is generally good, with most patient demonstrating clinical improvement upon normalization of blood glucose. In treatment refractory cases, neurosurgical intervention, such as deep brain stimulator implantation and pallidal surgery, could be considered and have demonstrated success in case reports.