Answer of March 2023
For completion of the online quiz, please visit the eHKAM LMS website or HKAM iCMECPD website.
Clinical History:
A 58-year-old man with history of prior abdominal surgery. Contrast enhanced CT shows a pancreatic tail lesion.
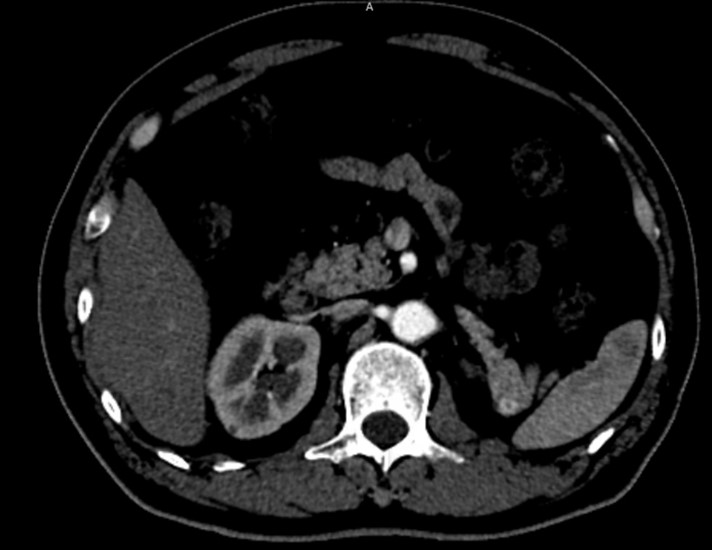
Contrast CT = Arterial phase
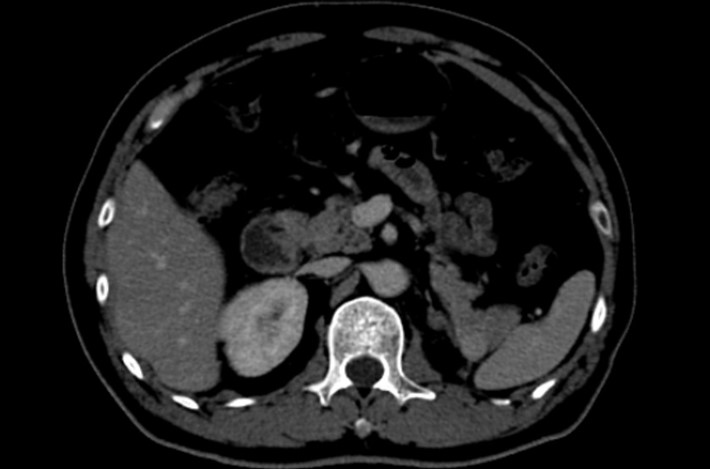
Contrast CT portovenous phase
DIAGNOSIS
Pancreatic tail metastasis from renal cell carcinoma, proven histologically after resection.
IMAGING FINDINGS
A new small arterial enhancing lesion, compared to pancreatic parenchyma, is seen at the pancreatic tail. It shows mild homogeneous hyper-enhancement on the portovenous phase. No calcifications seen nor relation to adjacent vessels.
No other pancreatic lesion was seen. The left kidney is not seen, consistent with history of left nephrectomy.
No hyper-enhancing lesions were seen in the rest of the abdomen.
DISCUSSION
Renal cell carcinoma (RCC) is the second most common urologic cancer with metastatic disease occurring in up to 18% at time of primary tumour diagnosis and 50% of patients developing on post nephrectomy follow-up.
Metastases of renal cell carcinoma (RCC) may result from haematogenous or lymphatic spread.
Contrast-enhanced CT should ideally use both arterial and nephrographic phases as subtypes can vary in the enhancement. Metastatic lesions tend to follow the same enhancement as the primary tumour.
The most common sites of metastatic are lungs, bone, lymph nodes, liver, adrenal glands and the brain.
Although metastatic spread to the pancreas is relatively rare, RCC has higher tendency than other cancers to do so. They usually develop several years after nephrectomy and may be the only site of metastasis.
On contrast enhanced CT, there is usually avid homogeneous hyperenhancement in the arterial phase compared to the normal pancreatic parenchyma. Larger lesions may show areas of central necrosis.
The main imaging differentials include intra-pancreatic accessory spleen, solid pseudopapillary tumour, splenic artery aneurysm or pseudoaneurysm and solid serous cystadenoma of the pancreas. Intra-pancreatic accessory spleen is usually seen as a well-defined hyper-vascular lesion, in the tail of the pancreas. Its CT attenuation and pattern of enhancement follows that of the spleen, with heterogeneous enhancement on arterial phase. Solid pseudopapillary neoplasm almost only occurs in young women below the age of 40 years old. Imaging appearances typically as a well-defined solid heterogeneous mass owing to internal hemorrhage and necrosis. Splenic artery aneurysm or pseudoaneurysm, direct communication with vessel and sometimes peripheral calcifications and/or mural thrombus may be seen. Solid serous cystadenoma of the pancreas can appear solid in a minority of cases due to closely apposed enhancing septa and walls. They tend to show lobulated margin and a central scar or calcification may be identified.