Answer of January 2022
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A 49-year-old female with a history of hypothyroidism and hypercalcemia.
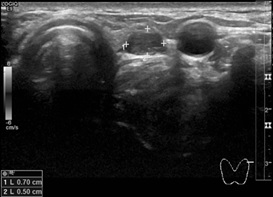

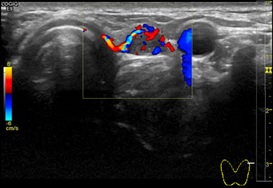
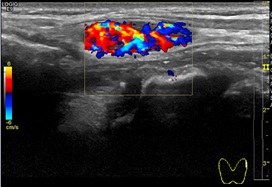
Thyroid ultrasound

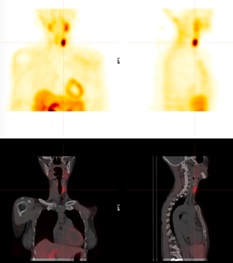
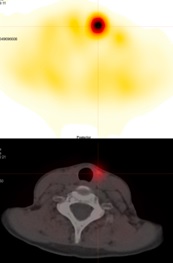
Selected images of Tc-99m Sestamibi scintigraphy
IMAGING FINDINGS
Ultrasound thyroid: a circumscribed gently lobulated hypoechoic nodule noted posterior to the upper pole of the left thyroid gland, measuring 0.7 cm × 0.5 cm × 2.4 cm. Markedly increased vascularity of the lesion detected.
Tc-99m Sestamibi scintigraphy: early images at 10 min showed an elongated oval area of homogeneous increased tracer uptake on the left side of the trachea, over the region of the left lobe of the thyroid. No uptake in the right thyroid bed. No abnormal uptake in the rest of the neck. No MIBI-avid lesion in the thorax. Delayed images at 2 hours showed persistent homogeneous tracer uptake in the lesion mentioned above over the left lobe of the thyroid. No uptake in the rest of the neck, including right thyroid bed. No MIBI-avid lesion was found in the thorax.
DIAGNOSIS
Left parathyroid adenoma.
DISCUSSION
Parathyroid adenoma is a benign tumor of the parathyroid gland and is the most common cause of primary hyperparathyroidism. Patients with primary hyperparathyroidism present with elevated serum calcium and parathyroid hormone levels, but most do not have symptoms. When symptoms appear, they are multisystem presentations, including osteoporosis, urolithiasis, constipation, peptic ulcers, mental changes, and depression.
Sonography and 99mTc-sestamibi scintigraphy are the dominant imaging techniques for the preoperative location of parathyroid adenomas. Numerous studies comparing these techniques suggest similar sensitivities and specificities for solitary adenoma detection. In recent years, 4D parathyroid CT has emerged as a valuable modality to precisely localize adenomas preoperatively, and it has been shown to be more sensitive than sonography and scintigraphy for preoperative localization by many studies. MRI is infrequently utilized in initial workup because of lower spatial resolution and artifacts. Contrast-enhanced CT and MRI are more commonly used to detect suspected ectopic—often mediastinal—glands.
Parathyroid adenomas are usually oval or bean-shaped. Most adenomas are solitary lesions. On ultrasound, they are nearly always homogeneously hypoechoic to the overlying thyroid gland on grey-scale imaging. Internal vascularity is commonly seen in a peripheral distribution. The artery feeding the adenoma tends to branch around the periphery of the gland before penetrating deeper, resulting in a characteristic arc or rim of vascularity.
Sestamibi with 99mTc is the most commonly used radiotracer for imaging the parathyroid glands. Sestamibi is taken up by both the thyroid and parathyroid glands, but adenomatous and hyperplastic parathyroid tissue shows more avid uptake of the radiotracer and often retains the radiotracer longer than adjacent thyroid tissue. Thus, early planar images obtained shortly after the administration of radiotracer will show both thyroid and parathyroid tissue. Asymmetric foci of increased radiotracer uptake on early images can be seen, representing abnormal parathyroid tissue superimposed on the normal thyroid. Delayed images, obtained approximately 2 hours after radiotracer administration, are acquired to look for foci of retained radiotracer characteristic of hyperfunctioning parathyroid tissue.
Surgery is the choice of treatment, and it is successful in treating primary hyperparathyroidism caused by parathyroid adenomas in 95-98% of cases. However, in our case, the patient was incidentally found to have hypercalcemia and elevated parathyroid hormone level, and clinically asymptomatic. So, she was not offered surgical parathyroidectomy.