Answer of October 2018
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A young female patient in her mid-thirties and with good past health presents with a right facial lump which has been waxing and waning in size for years, and occasionally painful. No skin changes, skin defect or abnormal discharge.
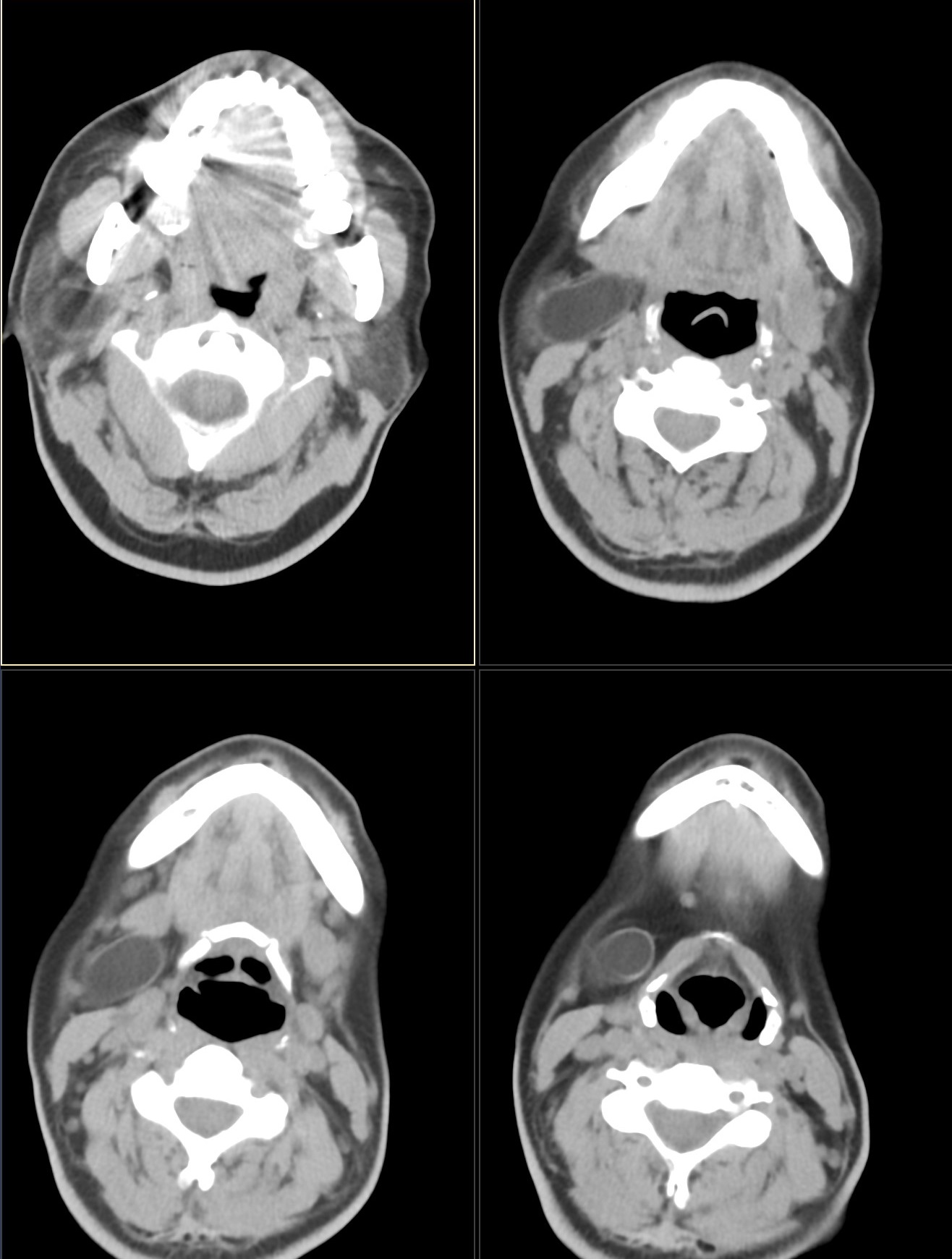
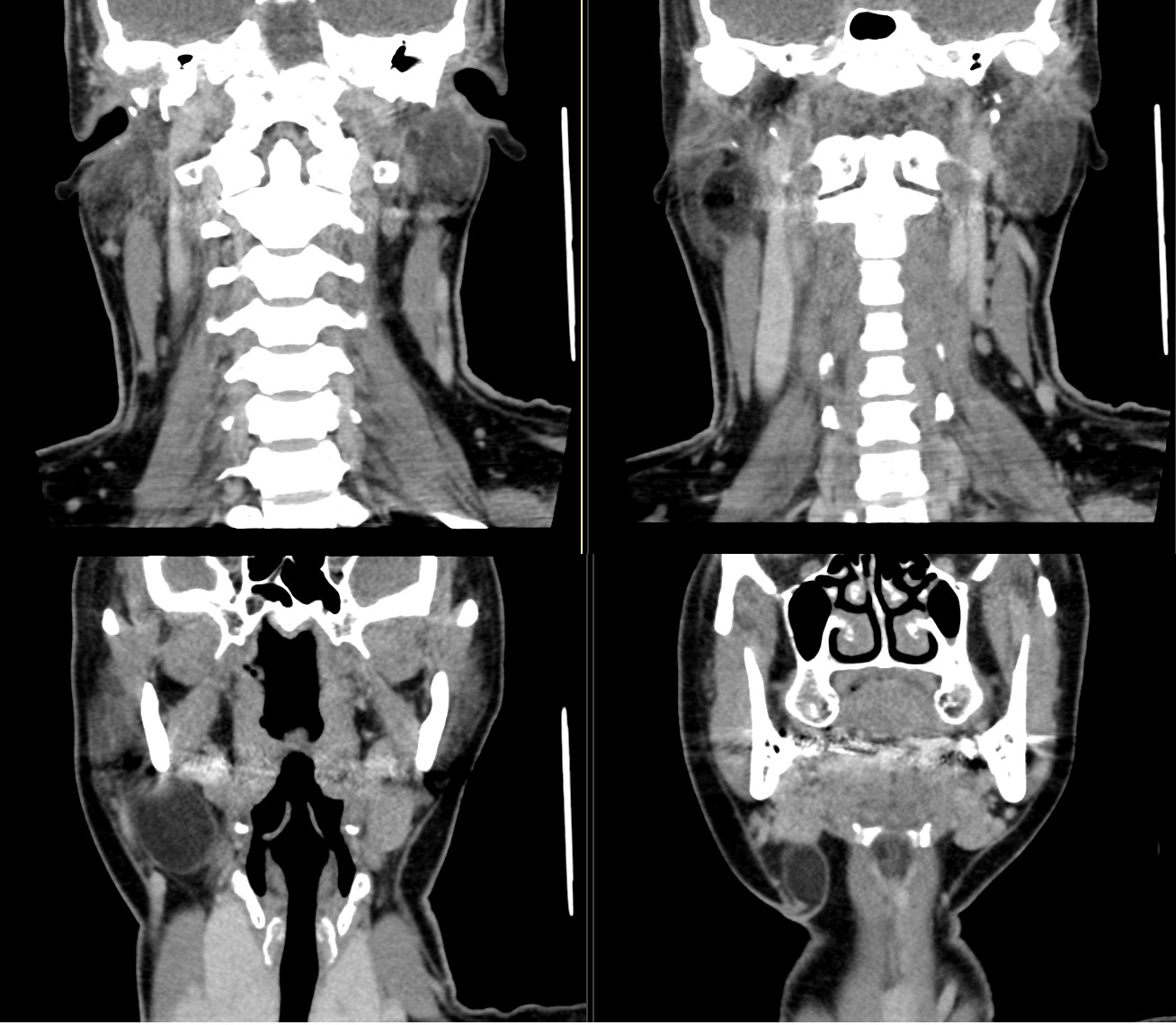
Contrast CT images of the head and neck are shown.
Imaging Findings:
Contrast CT shows a thin rim-enhancing cystic lesion extending from the deep lobe of the right parotid gland into the right parapharyngeal space, with a narrow portion leading towards the skin at the right submandibular region above the level of the hyoid bone. It is not closely related to the larynx.
Discussion:
Cystic lesions of the neck are usually diagnosed in infancy and childhood, although some present in adulthood. Vast majority are congenital. Differential diagnoses include thyroglossal duct cysts, branchial cleft cysts, cystic hygromas, dermoid and epidermoid cysts, thymic and bronchogenic cysts, and larygocoeles. Thyroglossal duct cysts, branchial cleft cysts and cystic hygromas are the three most common entities to present as a cystic mass in the neck.
Branchial cleft abnormalities as a group are the second commonest cause of congenital cystic neck masses. Six branchial arches separated by five pairs of ectodermal clefts and five endodermal branchial pouches are present during embryonic life. Branchial cleft abnormalities occur as persistent remnants of these structures and may manifest as cysts, fistulas, sinuses, or skin tags.
The first branchial cleft cyst arises from the remnant of the first branchial cleft or arch extending from the external auditory canal through the parotid gland to the submandibular triangle. 1st branchial cleft cysts are uncommon and account for only about 5% of branchial cleft abnormalities, and are most commonly seen in middle-aged women. They often manifest as recurrent abscesses or other inflammation around the ear or angle of mandible. Patient typically has a history of recurrent parotid abscesses despite treatment. Otorrhoea can occur if the lesion drains into the external auditory canal.
Work divided first branchial cleft cysts into two types. Work Type 1 cysts are derived from ectoderm and represent a duplication anomaly of the membranous external auditory canal, and are typically found medial to the concha of the ear and may extend into the retroauricular area. Work type 2 cysts arise from the ectoderm and mesoderm, and can involve the external auditory canal and cartilaginous pinna. The presence of mesoderm derived skin appendages (hair follicles, sweat and sebaceous glands) allow differentiation from Work type 1 cysts.
First branchial cleft cysts associated with the parotid gland are normally classified as Work type 2 cysts. They can be distinguished histologically from parotid lymphoepithelial cysts, which lack mesodermal components.
Second branchial cleft abnormalities account for the majority (95%) of branchial cleft abnormalities, and are mostly cysts. Majority of these cysts occur along the anterior surface of the sternocleidomastoid muscle.
Thickening and
enhancement of the cyst wall is usually due to inflammation.
Complete excision is the only curative treatment for branchial cleft cysts.
Dermoid and epidermoid cysts arise from sequestration of skin-forming cellular elements. The essential difference between a dermoid cyst and epidermoid cyst lies in the presence of skin appendages (sebaceous glands and hair follicles) in the wall of a dermoid cyst and their absence in epidermoid cysts. Head and neck region dermoid cysts manifest in the 2nd-3rd decades of life, most commonly at the lateral eyebrow, followed by the floor of mouth. Epidermoid cysts are much rarer than dermoid cysts in the neck.
Cystic hygromas are usually detected in the first 2 years of life. They arise from the sequestration of embryonic lymphatic channels. Most of these occur in the posterior triangle of the neck, followed by the oral cavity. In adults, they are seen more commonly in the sublingual, submandibular and parotid glands. The most characteristic feature of cystic hygromas is their infiltrative appearance, with a lack of respect for any fascial planes.
Laryngocoeles arise from the laryngeal saccule, which is a mucosa-line pouch along the roof of the laryngeal ventricle, an orifice located between the true and false vocal cords. They are though to develop due to an increase in supraglottic pressure in relation to voice abuse. These can be classified as internal, external or mixed. External laryngocoeles extend through the thyrohyoid membrane at the point of insertion of superior laryngeal nerve and vessels, while internal laryngocoeles are confined to the larynx. Mixed laryngocoeles contain external and internal components.
Thyroglossal duct cysts are the most common congenital neck mass, and account for 70% of congenital neck anomalies. They are remnants of the thyroglossal duct, which can be traced from the foramen caecum of the tongue to the pyramidal lobe of the thyroid gland, with a path which pierces the thyrohyoid membrane. However, they are usually located in the midline or paramedian location and closely associated with the anterior aspect of the hyoid bone or within the strap muscles.