| ||||||||||||

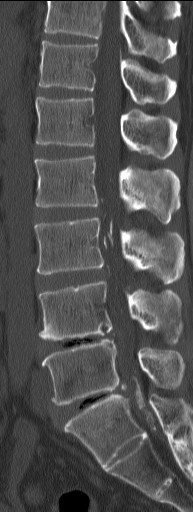


CLINICAL HISTORY: A middle age man presented with lower limb weakness DIAGNOSIS:Arachnoiditis ossificans DISCUSSION:Arachnoiditis ossificans is a rare condition in which there is intradural ossification associated with post inflammatory adhesion and clumping of nerve roots. Usually it affects the lumbosacral or the thoracic region. Common presenting symptoms are progressive lower limb weakness, numbness, and incontinence. Causes include trauma, surgery, subarachnoid haemorrhage, myelography, infection, and spinal anaesthesia. An association with syringomyelia is documented. This entity is hardly diagnosed with radiograph and myelography due to obscuration of the ossification by overlapping structures and intrathecal contrast respectively. CT is the imaging of choice, which shows calcified and/ or ossified densities within clumped nerve roots. At the lumbosacral region calcification surrounding conus medullaris and cauda equina might be evident. In MRI, the clumped nerve roots form cord and mass like structures. Their signal intensities are variable in both T1W and T2W images, and with variable contrast enhancement. Intraspinal cysts and loculation might be present. The prognosis is variable. While some have progressive compressive myelopathy, the rest remain stable with only mild symptoms, regardless of the degree of ossification. The best treatment strategy has not been established. There is no proven therapeutic advantage in resecting intradural ossifications. Decompressive laminectomy over entire length of ossification has some reported success. |
||
PREVIOUS CASES |
||
HOME |
COMMENTS |
|