CLINICAL HISTORY:
A 22 year-old female patient with a history of scalp swelling since young complained of a scalp mass with bony defect at skull vertex. CT, MRI and DSA were performed.
DIAGNOSIS:
Sinus pericranii (closed type)
DISCUSSION:
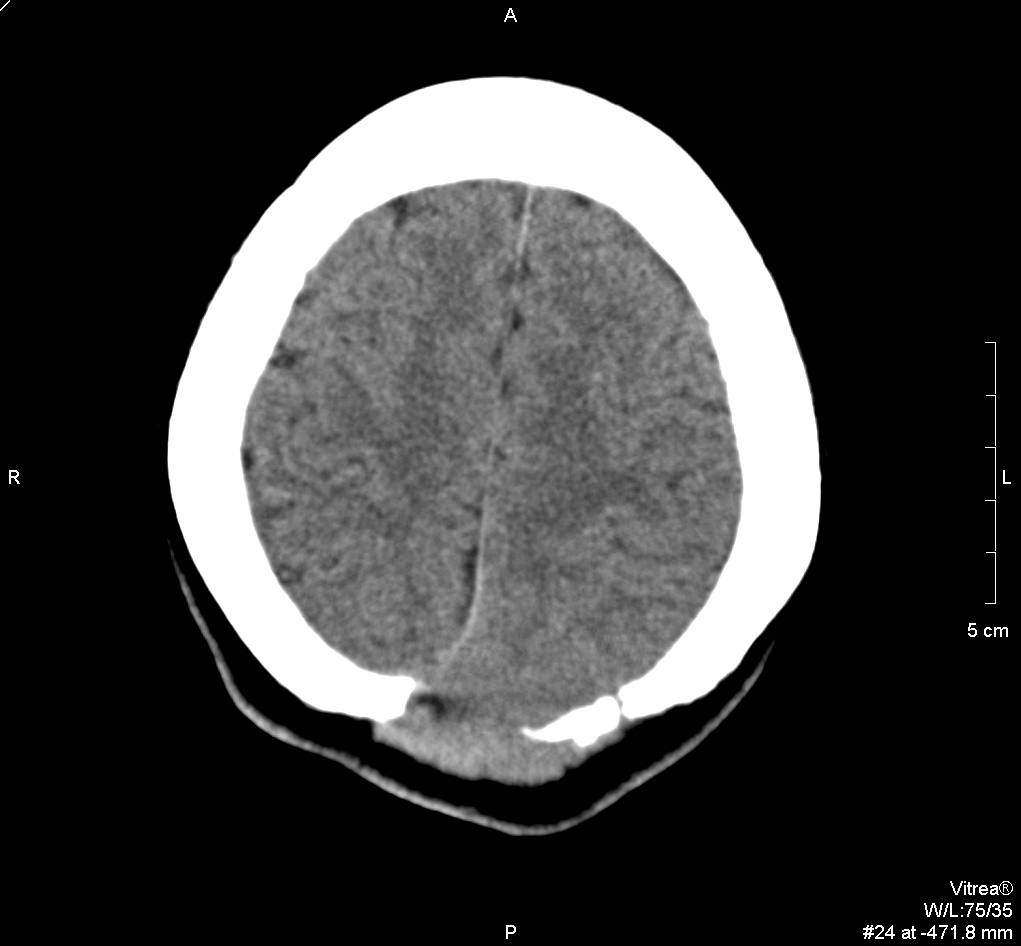
CT brain showed a bony defect in the left parietal parasagittal area,
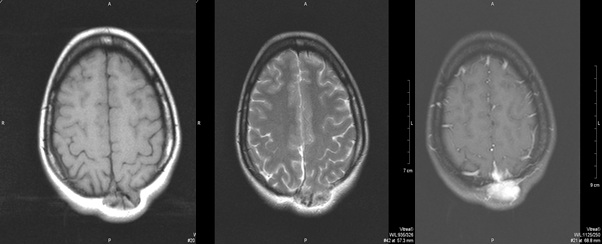
associated with an extracranial soft tissue lesion. MRI brain revealed a
lobulated extra-axial heterogenous enhancing lesion in the left parietal
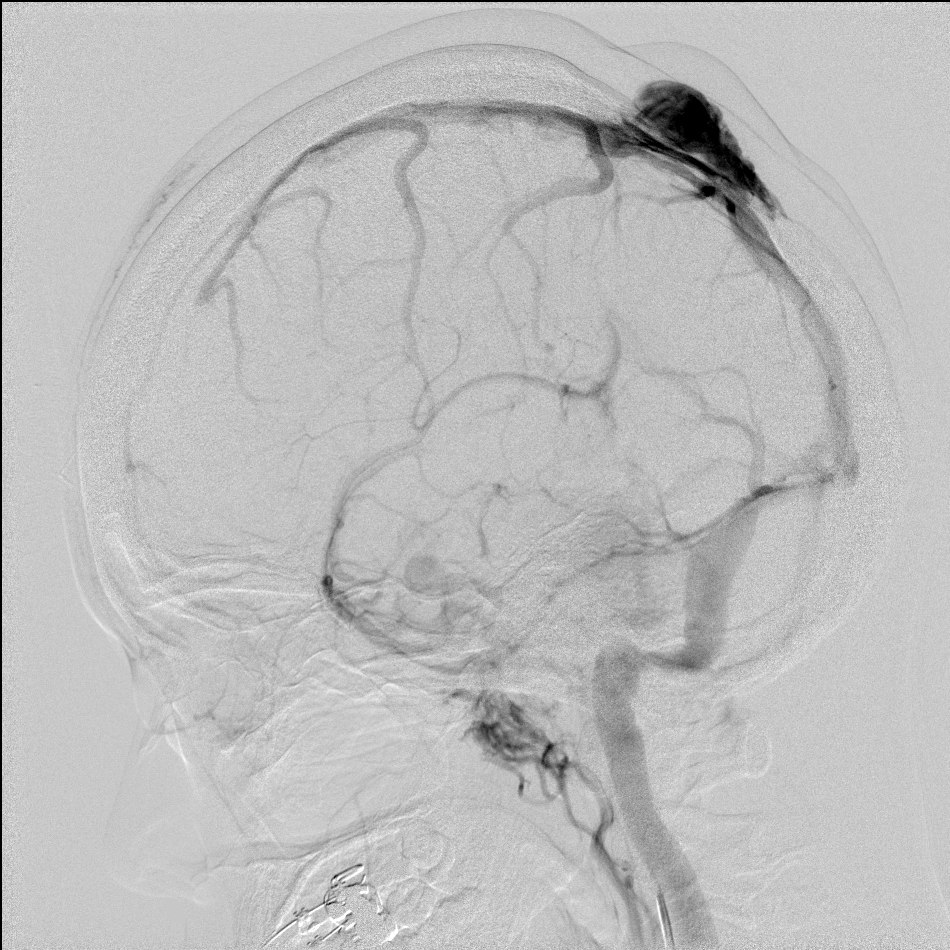
region. DSA demonstrated a venous pouch at the left parietal scalp region in
parasagittal location, which is supplied and drained through the superior
sagittal sinus. Overall features are suggestive of sinus pericranii (closed
type).
Sinus pericranii is an unusual venous anomaly characterized by collection of
venous blood vessels adhering to the outer surface of the skull,
communicating with dural venous sinus and extracranial venous system (venous
varix & venous malformation). The condition is featured as a vascular scalp
mass communicating with dural venous sinus via transcalvarial vein, which
courses through a well defined bony defect. Most frequently it is at the
frontal or parietal region around midline or paramedian in location, with
superior sagittal sinus most commonly involved.
Sinus pericranii can be classified as "closed" and "drainer" types based on
the venous drainage pattern. Closed type: blood comes from and drains into
dural venous sinus. Drainer type: blood comes from dural venous sinus, and
drains into scalp veins.
Symptoms are infrequent but include headache, vertigo, feelings of fullness,
or local pain. A non-tender fluctuant bluish scalp mass can be detected,
which reduces in upright position and distends when lying prone or with
Valsalva maneuver.
Most lesions are congenital, but traumatic causes with disruption of
emissary veins at outer table are also possible. They can be associated with
developmental venous anomalies, systemic venous malformations, blue rubber
bleb nevus syndrome and multisutural craniosynostosis.
Treatment options include surgery and endovascular therapy. Surgery is
usually done for symptomatic cases with the aim of cosmetic improvement.
Removal of extracranial venous component, ligation of transosseous emissary
veins with closure of bone holes / cranioplasty are performed. Good
prognosis is usually achieved after surgical removal, and recurrence is
uncommon. Endovascular therapy can be given with percutaneous injection of
sclerosants or coils into the draining scalp veins, and is usually reserved
for small or single drainer sinus pericranii. However, treatment is
contraindicated if the sinus pericranii serves as a major intracranial
venous drainage pathway or drains an underlying developmental venous
anomaly.
|