|
|
|
|
|
|

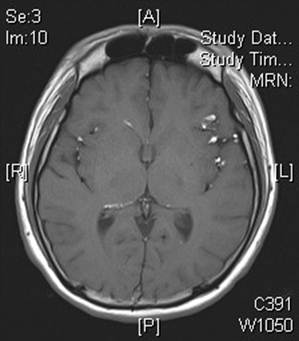
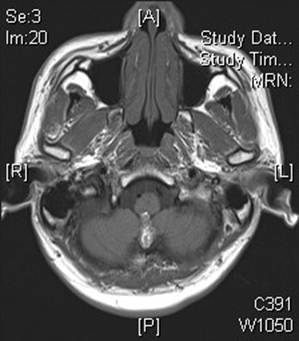
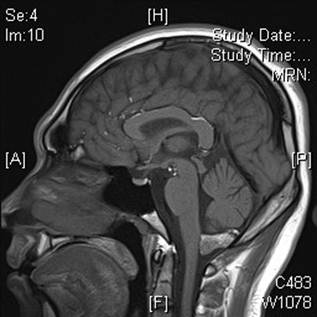
CLINICAL HISTORY: DIAGNOSIS: DISCUSSION: Dermoid cysts are lined by stratified squamous epithelium and may have hair follicles, sweat and sebaceous gland components. Glandular secretion and epithelial desquamation causes these cysts to enlarge and rupture, the latter inducing a chemical meningitis which triggers vasospasm, infarction and sometimes death. Malignant transformation into squamous cell carcinoma has also been described. Dermoid cysts are often misconceived to arise from both ectodermal and mesodermal elements. In fact, their origin is strictly ectodermal. Dermoid cysts arise from inclusion of ectodermally committed cells at the time of neural tube closure, and are inclusion cysts. Its capsule consists of simple epithelium supported by collagen, and in thicker parts, contains dermal elements including hair follicles, sebaceous and sweat glands. Despite the name, they are completely distinct from ovarian dermoid cysts, which are mature cystic teratomas. Imaging findings vary, depending on whether the cyst has ruptured. Unruptured cysts have the same imaging characteristics as fat because they contain liquid cholesterol. All are hyperintense on T1-weighted images and do not enhance. The masses have heterogeneous signal intensity on T2-weighted MR images and vary from hypo- to hyperintense. The best diagnostic clue of a ruptured dermoid cyst is fatlike droplets in the subarachnoid cisterns, sulci, and ventricles. Extensive pial enhancement can be seen from chemical meningitis caused by ruptured cysts. Treatment for ruptured intracranial dermoid cyst varies. While many clinicians adopt a conservative approach, others opt for early tumour resection and attempted irrigation of the subarachnoid space. External ventricular drainage may be required when there is hydrocephalus. Dermoid cysts may be confused with an epidermoid, craniopharyngioma, teratoma, or lipoma. Epidermoid cysts typically resemble CSF (not fat), lack dermal appendages, less likely to calcify, and are usually located off midline. Like dermoid cysts, craniopharyngiomas are suprasellar, with a midline location, and demonstrate nodular calcification. However, most craniopharyngiomas are strikingly hyperintense on T2-weighted images and enhance strongly. Teratomas may also have a similar location but usually occur in the pineal region. Lipomas demonstrate homogeneous fat attenuation and/or signal intensity and show a chemical shift artifact, which typically does not occur with dermoid cysts. |
||
PREVIOUS CASES |
||
HOME |
COMMENTS |
|